LEEP ve Konizasyon: Rahim Ağzı Hücre Değişikliklerinde Tanı, Tedavi ve Takip
Rahim ağzı, yani serviks, rahmin vajinaya açılan alt bölümüdür. Bu bölgede özellikle HPV enfeksiyonu ile ilişkili hücresel değişiklikler gelişebilir. Bu değişikliklerin bir kısmı kendiliğinden gerileyebilirken, bazıları zaman içinde kanser öncüsü lezyonlara dönüşebilir. LEEP ve konizasyon, rahim ağzındaki anormal veya kanser öncüsü dokuların çıkarılması için kullanılan önemli işlemlerdir.
Peki her anormal smear sonucu kanser anlamına mı gelir?
Hayır. Anormal smear veya HPV pozitifliği çoğu zaman kanser anlamına gelmez. Bu sonuçlar, rahim ağzındaki hücrelerde değişiklik olabileceğini ve daha ayrıntılı değerlendirme gerektiğini gösterir. Amaç, kanser gelişmeden önce riskli hücreleri saptamak ve gerekli durumlarda tedavi etmektir.
LEEP nedir?
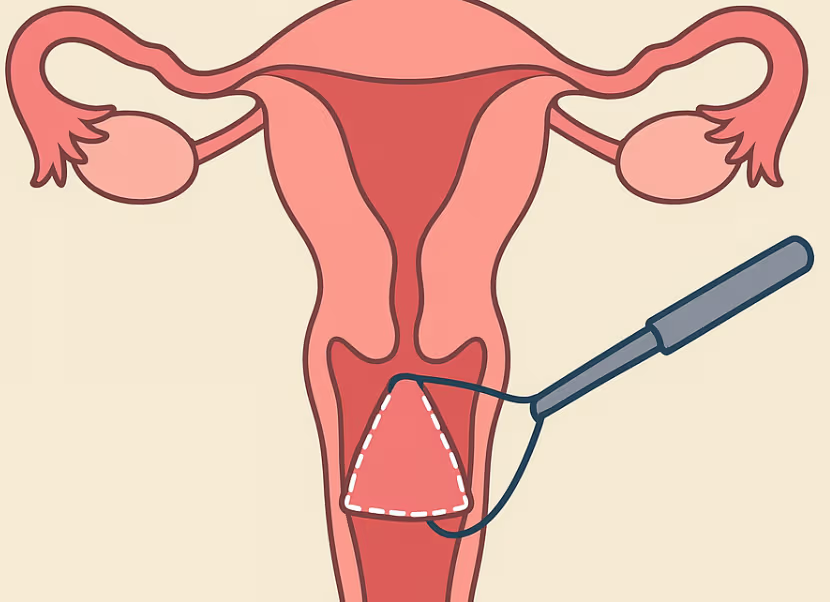
LEEP, İngilizce “Loop Electrosurgical Excision Procedure” ifadesinin kısaltmasıdır. Türkçede elektrik akımı taşıyan ince bir tel halka ile rahim ağzındaki anormal dokunun çıkarılması olarak açıklanabilir. İşlem sırasında rahim ağzındaki şüpheli alan çıkarılır ve patolojik incelemeye gönderilir.
LEEP genellikle şu durumlarda uygulanır:
Kolposkopi ve biyopsi sonucunda CIN 2 veya CIN 3 gibi yüksek dereceli rahim ağzı hücre değişiklikleri saptandığında
Smear, HPV testi ve biyopsi sonuçları birlikte değerlendirildiğinde tedavi gerektiren risk görüldüğünde
Rahim ağzındaki anormal alanın hem tedavi edilmesi hem de patolojik olarak değerlendirilmesi istendiğinde
LEEP çoğunlukla ayaktan yapılabilen, kısa süren ve lokal anestezi ile uygulanabilen bir işlemdir. Uygun hastalarda hem tanı hem tedavi amacı taşır.
Konizasyon nedir?
Konizasyon, rahim ağzından koni şeklinde bir doku parçasının çıkarılmasıdır. Bu işlem “kon biyopsi” olarak da adlandırılır. Çıkarılan doku, rahim ağzının yüzeyini ve rahim ağzı kanalına uzanan bölümü içerebilir. Böylece daha geniş ve derin bir patolojik değerlendirme yapılabilir.
Konizasyon şu durumlarda tercih edilebilir:
Kolposkopide lezyonun tamamı görülemiyorsa
Anormal hücrelerin rahim ağzı kanalına doğru uzandığı düşünülüyorsa
Smear, HPV, kolposkopi ve biyopsi sonuçları arasında uyumsuzluk varsa
Glandüler hücre anormalliği veya adenokarsinoma in situ şüphesi varsa
Mikroinvaziv kanser olasılığını dışlamak veya değerlendirmek gerekiyorsa
Önceki tedaviden sonra sınırlar veya hastalığın yaygınlığı net değilse
Konizasyon soğuk bıçak yöntemiyle, lazerle veya bazı durumlarda LEEP tekniğiyle yapılabilir. Günlük kullanımda “konizasyon” denildiğinde çoğu zaman soğuk bıçak konizasyonu kastedilir.
LEEP ile konizasyon arasındaki fark nedir?
LEEP ve konizasyonun ortak yönü, her ikisinin de rahim ağzından doku çıkararak hem tedavi hem de patolojik inceleme imkânı sağlamasıdır. Ancak aralarında bazı önemli farklar vardır.
LEEP genellikle daha yüzeyel veya sınırlı alanların çıkarılmasında kullanılır. Çoğu zaman poliklinik koşullarında ve lokal anestezi ile yapılabilir. İşlem süresi kısadır ve iyileşme genellikle hızlıdır.
Konizasyon ise daha geniş veya derin doku çıkarılması gereken durumlarda tercih edilir. Özellikle lezyon rahim ağzı kanalına uzanıyorsa, kolposkopi yetersizse veya kanser şüphesi daha dikkatli değerlendirilmeliyse konizasyon daha uygun olabilir. Soğuk bıçak konizasyonunda doku kenarları ısı etkisinden daha az etkilendiği için patolojik sınır değerlendirmesi bazı durumlarda daha net yapılabilir.
Kısaca: LEEP çoğu yüksek dereceli rahim ağzı hücre değişikliğinde etkili ve daha pratik bir tedavi seçeneğidir. Konizasyon ise daha derin, daha geniş veya tanısal açıdan daha hassas değerlendirme gereken durumlarda öne çıkar.
Bu hastalık belirti verir mi?
Rahim ağzındaki kanser öncüsü hücre değişiklikleri çoğu zaman belirti vermez. Bu nedenle düzenli smear ve HPV taraması çok önemlidir. Hastalar genellikle herhangi bir şikâyeti olmadan, rutin tarama sonucunda anormal bulgu ile değerlendirmeye alınır.
Bazen altta yatan rahim ağzı hastalıklarında şu şikâyetler görülebilir:
İlişki sonrası kanama
Adet dışı lekelenme veya kanama
Menopoz sonrası kanama
Kötü kokulu veya olağandışı vajinal akıntı
Pelvik ağrı
Bu belirtiler mutlaka kanser anlamına gelmez; enfeksiyon, polip, hormonal nedenler veya başka jinekolojik durumlarla da ilişkili olabilir. Ancak özellikle tekrarlayan veya açıklanamayan kanamalarda jinekolojik değerlendirme gerekir.
Tanı nasıl konur?
Tanı genellikle birkaç basamakla konur:
İlk basamak smear testi ve/veya HPV testidir. Smear testi rahim ağzındaki hücrelerin mikroskop altında değerlendirilmesini sağlar. HPV testi ise rahim ağzı kanseriyle ilişkili yüksek riskli HPV tiplerinin varlığını araştırır.
Anormal sonuç saptanırsa kolposkopi yapılabilir. Kolposkopi, rahim ağzının özel bir büyütme sistemi ile ayrıntılı incelenmesidir. Şüpheli alanlardan biyopsi alınabilir. Gerekli durumlarda rahim ağzı kanalından örnekleme de yapılabilir.
LEEP veya konizasyon ise bazı hastalarda tanının kesinleştirilmesi ve aynı seansta tedavi sağlanması için uygulanır. Çıkarılan dokunun patolojik incelemesi, lezyonun derecesini, sınırlarını ve kanser şüphesi olup olmadığını belirlemede çok değerlidir.
Tedavi nasıl seçilir?
Tedavi kararı tek bir teste göre verilmez. Hastanın yaşı, gebelik planı, smear sonucu, HPV tipi, kolposkopi bulguları, biyopsi sonucu, lezyonun yeri ve önceki takip öyküsü birlikte değerlendirilir.
Düşük dereceli hücre değişikliklerinde her zaman hemen işlem gerekmez. Bazı hastalarda takip yeterli olabilir. Çünkü özellikle genç hastalarda hafif değişiklikler zamanla gerileyebilir.
Yüksek dereceli değişikliklerde ise LEEP veya konizasyon gibi eksizyonel tedaviler tercih edilebilir. Amaç, kanser öncüsü dokuyu çıkarmak ve aynı zamanda patolojik olarak ayrıntılı incelemektir.
İşlem sonrası neler normaldir?
LEEP veya konizasyon sonrası birkaç gün ile birkaç hafta arasında hafif kasık ağrısı, adet sancısına benzer kramp, lekelenme, kahverengi-siyah akıntı veya sulu akıntı olabilir. Bunlar çoğu zaman iyileşme sürecinin parçasıdır.
Hekimin önerdiği süre boyunca cinsel ilişkiden, tampon kullanımından, vajinal duş uygulamalarından, havuzdan ve ağır egzersizden kaçınmak gerekebilir. Bu süre genellikle birkaç haftadır ancak işlemin tipine ve hastanın durumuna göre değişebilir.
Hangi durumlarda doktora başvurulmalıdır?
İşlem sonrası şu durumlarda vakit kaybetmeden hekime başvurulmalıdır:
Yoğun kanama
Kötü kokulu akıntı
Ateş
Şiddetli kasık veya karın ağrısı
Ağrı kesiciye rağmen geçmeyen ağrı
Baş dönmesi, baygınlık hissi veya genel durumda bozulma
Bu bulgular enfeksiyon, kanama veya başka bir komplikasyon açısından değerlendirme gerektirebilir.
Takip neden bu kadar önemlidir?
LEEP veya konizasyonla anormal doku çıkarılsa bile takip tamamlanmış sayılmaz. Çünkü HPV enfeksiyonu devam edebilir veya anormal hücre değişiklikleri zaman içinde tekrarlayabilir. Bu nedenle işlem sonrası smear, HPV testi veya birlikte test ile düzenli kontrol gerekir.
Takip sıklığı; patoloji sonucuna, cerrahi sınırların temiz olup olmamasına, HPV sonucuna, hastanın yaşına ve önceki öyküsüne göre belirlenir. Yüksek dereceli lezyon tedavisi gören hastalarda uzun süreli takip özellikle önemlidir.
Gebelik planı olan hastalar için neden ayrıca değerlendirme gerekir?
LEEP ve konizasyon rahim ağzından doku çıkarılan işlemlerdir. Çoğu hasta ileride sorunsuz gebelik yaşayabilir. Ancak özellikle daha derin veya tekrarlayan işlemler rahim ağzı yetmezliği, erken doğum veya servikal darlık gibi riskleri artırabilir. Bu nedenle gebelik planı olan hastalarda tedavi kararı kişiye özel verilmelidir.
Sonuç
LEEP ve konizasyon, rahim ağzı kanseri gelişmeden önce riskli hücre değişikliklerini tanımak ve tedavi etmek için kullanılan değerli yöntemlerdir. LEEP daha pratik ve çoğu zaman daha sınırlı bir eksizyon sağlarken, konizasyon daha geniş veya derin değerlendirme gereken durumlarda tercih edilir. En doğru yaklaşım; smear, HPV testi, kolposkopi, biyopsi ve hastanın kişisel riskleri birlikte değerlendirilerek belirlenir.
Düzenli tarama, doğru tanı, uygun tedavi ve düzenli takip; rahim ağzı kanserinden korunmanın en etkili yollarındandır.
Bu yazı genel bilgilendirme amacı taşır. Tanı ve tedavi kararı için mutlaka kadın hastalıkları ve doğum uzmanı tarafından kişisel değerlendirme yapılmalıdır.