Endometrium Kanseri - Rahim Kanseri: Belirtiler, Tanı, Tedavi ve Takip Süreci
Endometrium kanseri, rahmin iç tabakasından, yani endometriumdan kaynaklanan bir kanser türüdür. Halk arasında çoğu zaman “rahim kanseri” olarak bilinir. Rahim kanserlerinin önemli bir bölümünü endometrium kanseri oluşturur ve özellikle menopoz sonrası dönemde daha sık görülür.
Bu hastalık çoğu zaman erken dönemde belirti verir. Bu nedenle belirtilerin doğru fark edilmesi ve zamanında değerlendirilmesi, tedavi başarısı açısından büyük önem taşır.
Endometrium nedir?
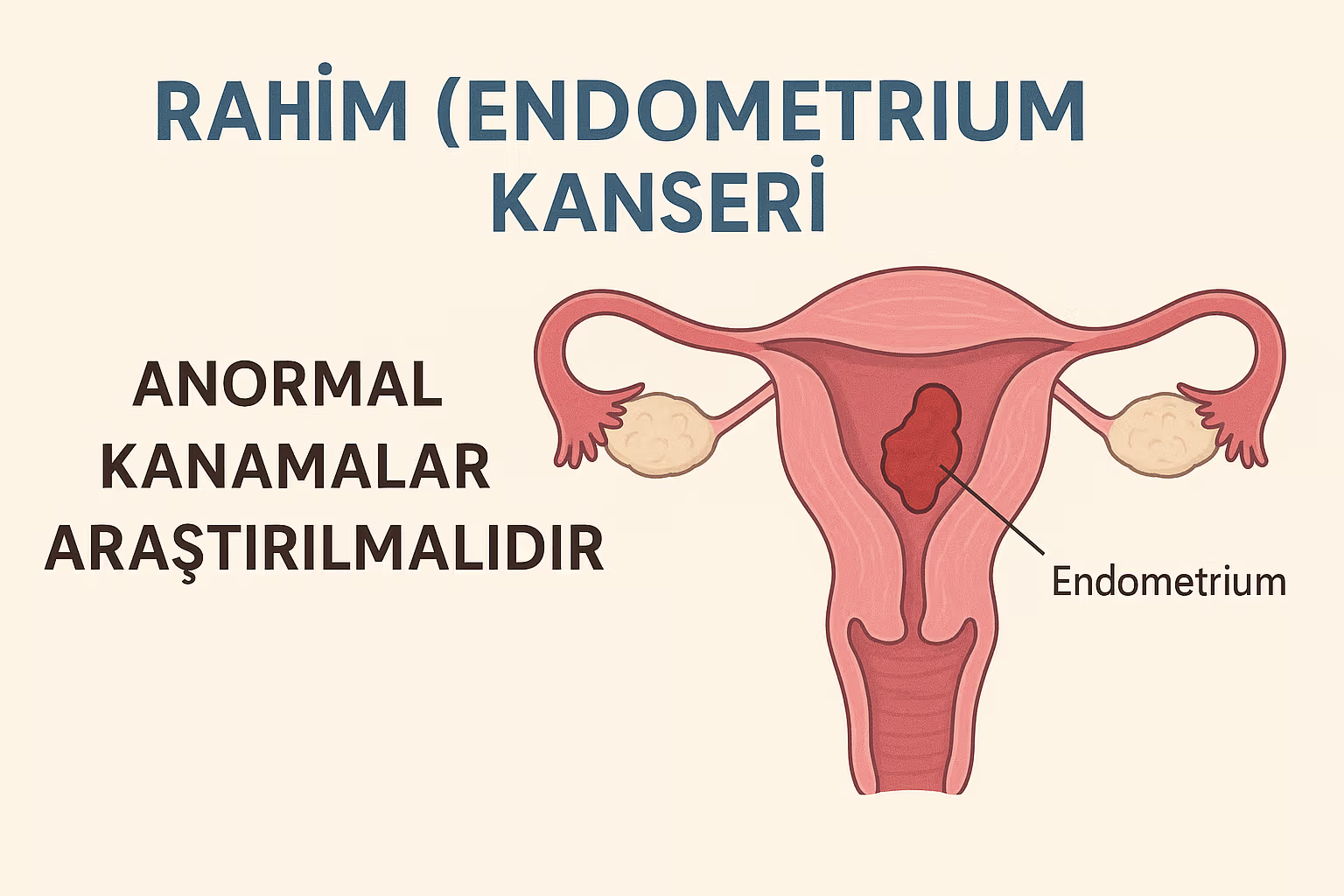
Endometrium, rahmin iç yüzeyini döşeyen dokudur. Üreme çağındaki kadınlarda hormonların etkisiyle her ay kalınlaşır ve gebelik oluşmazsa adet kanamasıyla birlikte dökülür. Menopozdan sonra ise hormon düzeyleri değiştiği için endometrium genellikle ince ve sakin bir yapıdadır.
Peki bu bilgi neden önemlidir?
Çünkü menopoz sonrası dönemde rahim içinden gelen herhangi bir kanama, “normal adet kanaması” olarak değerlendirilmemelidir. Bu durum mutlaka kadın hastalıkları ve doğum uzmanı tarafından incelenmelidir.
Endometrium kanseri kimlerde daha sık görülür?
Endometrium kanseri en sık menopoz sonrası kadınlarda görülür. Ancak yalnızca ileri yaş hastalığı değildir; daha genç yaşlarda da ortaya çıkabilir.
Risk artışı ile ilişkili durumlar şunlardır:
Menopoz sonrası dönem
Obezite
Uzun süreli karşılanmamış östrojen etkisi
Polikistik over sendromu
Hiç doğum yapmamış olmak
Erken yaşta adet görmeye başlamak veya geç menopoza girmek
Diyabet ve hipertansiyon gibi metabolik hastalıklar
Ailede endometrium, kolon veya bazı diğer kanserlerin bulunması
Lynch sendromu gibi kalıtsal kanser sendromları
Meme kanseri tedavisinde kullanılan tamoksifen öyküsü
Endometrial hiperplazi, özellikle atipili hiperplazi öyküsü
Ancak unutulmamalıdır: Risk faktörü olan herkes endometrium kanseri olmaz. Aynı şekilde hiçbir belirgin risk faktörü olmayan kişilerde de hastalık gelişebilir.
En önemli belirti nedir?
Endometrium kanserinin en sık belirtisi anormal vajinal kanamadır.
Burada kritik soru şudur:
“Hangi kanama ciddiye alınmalıdır?”
Aşağıdaki durumlarda gecikmeden hekime başvurulmalıdır:
Menopoz sonrası tek damla bile olsa vajinal kanama
Adet dönemleri arasında kanama
Normalden daha yoğun veya daha uzun süren adet kanamaları
Kanlı, kahverengi veya sulu vajinal akıntı
Cinsel ilişki sonrası kanama
Pelvik bölgede ağrı veya basınç hissi
İleri evrelerde kilo kaybı, halsizlik veya karında şişlik
Özellikle menopoz sonrası kanama, aksi kanıtlanana kadar araştırılması gereken bir bulgudur. Kanamanın az olması, kısa sürmesi veya kendiliğinden geçmesi hastalık olmadığı anlamına gelmez.
Her anormal kanama kanser midir?
Hayır. Anormal kanamanın birçok iyi huylu nedeni olabilir. Polipler, miyomlar, hormonal düzensizlikler, endometrial atrofi, enfeksiyonlar veya bazı ilaçlar kanamaya yol açabilir.
Ancak önemli olan şudur: Kanamanın nedenini tahmin etmek yerine doğru yöntemlerle değerlendirmek gerekir. Çünkü endometrium kanseri erken yakalandığında tedavi şansı oldukça yüksektir.
Tanı nasıl konur?
Endometrium kanserinde tanı, yalnızca muayene veya ultrason ile kesinleştirilemez. Kesin tanı için rahim içinden doku örneği alınması ve patoloji incelemesi gerekir.
Tanı sürecinde kullanılan başlıca yöntemler şunlardır:
1. Jinekolojik muayene
Hastanın şikayetleri, yaşı, menopoz durumu, kullandığı ilaçlar, aile öyküsü ve ek hastalıkları değerlendirilir. Pelvik muayene ile rahim, vajina ve çevre yapılar incelenir.
2. Transvajinal ultrasonografi
Vajinal ultrason ile rahim, yumurtalıklar ve endometrium kalınlığı değerlendirilir. Menopoz sonrası dönemde endometriumun kalın görünmesi veya düzensiz olması ileri inceleme gerektirebilir.
Ancak ultrason tek başına kanseri dışlamak için her zaman yeterli değildir. Klinik şüphe varsa doku tanısı gerekir.
3. Endometrial biyopsi
Rahim iç tabakasından küçük bir doku örneği alınır. Bu işlem çoğu zaman poliklinik koşullarında yapılabilir. Alınan örnek patoloji laboratuvarında incelenir.
4. Histeroskopi
Histeroskopi, rahim içinin kamera ile doğrudan görülmesini sağlayan yöntemdir. Özellikle polip, fokal lezyon veya yetersiz biyopsi şüphesi varsa değerlidir. Gerekirse aynı seansta hedeflenen bölgeden biyopsi alınabilir.
5. Evreleme ve görüntüleme
Kanser tanısı konulduktan sonra hastalığın rahimle sınırlı olup olmadığı değerlendirilir. Bunun için manyetik rezonans görüntüleme (MR), bilgisayarlı tomografi, PET/BT veya diğer görüntüleme yöntemleri kullanılabilir. Hangi tetkikin gerekli olduğu hastanın klinik durumuna göre belirlenir.
Patoloji raporunda nelere bakılır?
Endometrium kanserinde tedavi planı yalnızca “kanser var” bilgisine göre yapılmaz. Patoloji raporu tedavinin yönünü belirleyen çok önemli bilgiler içerir.
Başlıca değerlendirilen özellikler:
Kanserin histolojik tipi
Tümörün derecesi, yani grade’i
Rahim kas tabakasına yayılım derinliği
Lenf damar boşluğu invazyonu varlığı
Rahim ağzı, tüpler, yumurtalıklar veya çevre dokulara yayılım
Lenf nodu tutulumu
Moleküler sınıflama ve belirteçler
Günümüzde endometrium kanserinde moleküler değerlendirme giderek daha önemli hale gelmiştir. Bu değerlendirme, hastalığın davranışını daha iyi anlamaya ve kişiselleştirilmiş tedavi planlamasına yardımcı olabilir.
Tedavi nasıl planlanır?
Endometrium kanserinde tedavi; hastanın yaşı, genel sağlık durumu, çocuk isteği, tümör tipi, evresi, grade’i, yayılım durumu ve moleküler özellikleri dikkate alınarak planlanır.
Tedavi genellikle multidisipliner bir yaklaşımla yürütülür. Jinekolojik onkoloji uzmanı, medikal onkolog, radyasyon onkoloğu, patolog ve radyolog bu sürecin önemli parçalarıdır.
Cerrahi tedavi
Endometrium kanserinde temel tedavi çoğu hastada cerrahidir.
Standart cerrahi genellikle şunları içerir:
Rahmin alınması
Tüplerin ve yumurtalıkların alınması
Gerekli hastalarda lenf nodlarının değerlendirilmesi
Karın içi yayılım açısından cerrahi gözlem ve örnekleme
Günümüzde uygun hastalarda kapalı cerrahi yöntemler, yani laparoskopik veya robotik cerrahi tercih edilebilir. Minimal invaziv cerrahi, uygun hastalarda daha az ağrı, daha kısa hastanede kalış ve daha hızlı iyileşme sağlayabilir.
Lenf nodu değerlendirmesinde bazı hastalarda sentinel lenf nodu yöntemi kullanılabilir. Bu yöntem, kanserin ilk yayılabileceği lenf nodlarının özel boyalar veya işaretleyiciler yardımıyla saptanıp çıkarılmasına dayanır.
Her hastaya kemoterapi gerekir mi?
Hayır. Endometrium kanserinde her hastaya kemoterapi verilmez.
Tedavi kararı hastalığın risk grubuna göre verilir. Erken evre, düşük riskli hastalarda cerrahi tek başına yeterli olabilir. Daha yüksek riskli hastalarda ise radyoterapi, kemoterapi, immünoterapi, hedefe yönelik tedavi veya bunların kombinasyonları gündeme gelebilir.
Radyoterapi hangi durumlarda kullanılır?
Radyoterapi, kanserin tekrarlama riskini azaltmak amacıyla kullanılabilir. Bazen vajinal brakiterapi şeklinde, bazen de dıştan ışın tedavisi şeklinde uygulanır.
Radyoterapi kararı; tümörün evresi, grade’i, rahim kasına yayılım derinliği, lenf damar invazyonu ve diğer risk faktörlerine göre verilir.
Kemoterapi, immünoterapi ve hedefe yönelik tedaviler
İleri evre, yüksek riskli veya tekrarlayan endometrium kanserlerinde sistemik tedaviler gerekebilir.
Bu tedaviler arasında:
Kemoterapi
İmmünoterapi
Hedefe yönelik ilaçlar
Hormon tedavileri
yer alabilir.
Son yıllarda özellikle tümörün moleküler özelliklerine göre immünoterapi ve hedefe yönelik tedavilerin önemi artmıştır. Bu nedenle bazı hastalarda tümör dokusunda ek moleküler testler istenebilir.
Çocuk isteği olan genç hastalarda rahim korunabilir mi?
Bazı çok seçilmiş erken evre ve düşük riskli hastalarda, çocuk isteği varsa rahmi koruyucu tedavi seçenekleri değerlendirilebilir. Bu yaklaşım her hasta için uygun değildir.
Genellikle yalnızca rahim iç tabakasıyla sınırlı, düşük dereceli, uygun histolojik tipte ve yayılım bulgusu olmayan hastalarda düşünülür. Bu durumda hasta çok yakın takip edilmelidir. Tedavi sürecinde hormon tedavileri, düzenli biyopsiler ve görüntüleme yöntemleri kullanılır.
Bu karar mutlaka jinekolojik onkoloji deneyimi olan merkezlerde, ayrıntılı bilgilendirme sonrası verilmelidir.
Tedaviden sonra takip neden önemlidir?
Endometrium kanseri tedavisi tamamlandıktan sonra takip süreci başlar. Takibin amacı, olası nüksleri erken fark etmek, tedaviye bağlı yan etkileri yönetmek, yaşam kalitesini artırmak ve hastanın genel sağlığını desteklemektir.
Takipte genellikle:
Düzenli hekim görüşmeleri
Jinekolojik muayene
Şikayetlerin değerlendirilmesi
Gerekli durumlarda görüntüleme ve laboratuvar testleri
yer alır.
Her hastaya aynı takip şeması uygulanmaz. Takip sıklığı hastalığın evresine, risk grubuna, aldığı tedavilere ve hastanın genel durumuna göre belirlenir.
Hangi belirtiler takipte önemlidir?
Tedavi sonrası dönemde aşağıdaki belirtiler olursa hekime haber verilmelidir:
Vajinal kanama veya lekelenme
Yeni başlayan pelvik ağrı
Karında şişlik
Nedeni açıklanamayan kilo kaybı
Uzun süren öksürük veya nefes darlığı
Bacaklarda şişlik
İdrar veya bağırsak alışkanlıklarında belirgin değişiklik
Geçmeyen halsizlik
Bu belirtiler her zaman kanserin tekrarladığı anlamına gelmez. Ancak değerlendirilmesi gerekir.
Yaşam tarzı ve destekleyici bakım
Endometrium kanseri tedavisi yalnızca ameliyat, ilaç veya radyoterapiden ibaret değildir. Hastanın fiziksel ve psikolojik iyilik hali de tedavinin önemli bir parçasıdır.
Sağlıklı kilo yönetimi, düzenli fiziksel aktivite, dengeli beslenme, diyabet ve hipertansiyon gibi hastalıkların kontrolü, sigaradan uzak durmak ve düzenli hekim kontrolleri genel sağlık açısından önemlidir.
Tedavi sürecinde cinsellik, menopoz belirtileri, yorgunluk, lenfödem, bağırsak ve idrar sorunları gibi konular da gündeme gelebilir. Bu şikayetler utanılacak konular değildir; uygun destekle yönetilebilir.
Sık sorulan sorular
Menopoz sonrası kanamam oldu, beklemeli miyim?
Hayır. Menopoz sonrası kanama mutlaka değerlendirilmelidir. Kanama az olsa veya bir kez olmuş olsa bile hekime başvurmak gerekir.
Smear testi endometrium kanserini gösterir mi?
Smear testi esas olarak rahim ağzı kanseri taraması için kullanılır. Endometrium kanserini güvenilir şekilde dışlamaz. Şüpheli durumlarda rahim içinden doku örneği alınması gerekir.
Ultrason normal çıktıysa kanser kesin dışlanır mı?
Her zaman hayır. Ultrason önemli bir değerlendirme aracıdır, ancak kesin tanı yöntemi değildir. Şikayetler ve klinik risk devam ediyorsa biyopsi gerekebilir.
Endometrium kanseri erken yakalanabilir mi?
Evet. Endometrium kanseri çoğu zaman anormal kanama ile erken belirti verir. Bu nedenle özellikle menopoz sonrası kanamaların gecikmeden değerlendirilmesi erken tanı açısından çok önemlidir.
Tedaviden sonra normal yaşama dönmek mümkün mü?
Birçok hasta tedavi sonrası günlük yaşamına dönebilir. Dönüş süresi yapılan tedaviye, hastanın genel sağlık durumuna ve ek tedavi gerekip gerekmediğine bağlıdır. Takip sürecinde fiziksel iyileşme kadar psikolojik destek de önemlidir.
Sonuç
Endometrium kanseri, erken belirti verebilen ve erken tanı konulduğunda başarıyla tedavi edilebilen bir jinekolojik kanser türüdür. En önemli uyarı işareti anormal vajinal kanamadır. Özellikle menopoz sonrası kanamalar asla ihmal edilmemelidir.
Doğru tanı, uygun cerrahi yaklaşım, gerektiğinde ek tedaviler ve düzenli takip ile hastaların önemli bir kısmında başarılı sonuçlar elde edilebilir.
Bu yazı genel bilgilendirme amacı taşır. Tanı, tedavi ve takip planı her hasta için bireysel olarak belirlenmelidir. Şikayetiniz veya risk faktörünüz varsa kadın hastalıkları ve doğum uzmanına başvurmanız önerilir