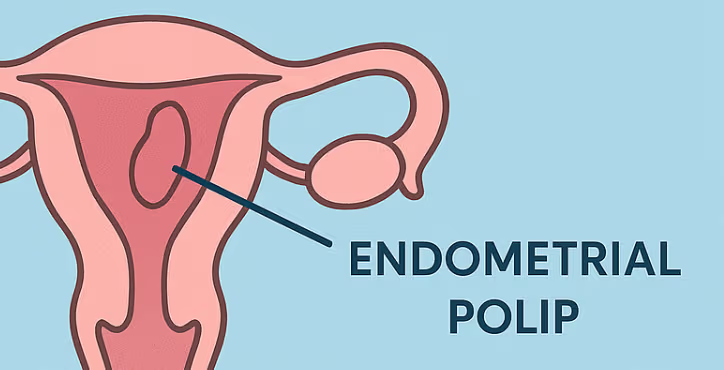
Endometrial polip rahim iç zarından köken alan iyi huylu oluşumdur. Adet düzensizlikleri ve aşırı kanamalara sebep olur. Tedavisinde polibin alınması gerekir.
Bunun için karından herhangi bir kesi yapılmadan, rahim ağzından kamera ile girilerek polip alınır (histeroskopi ameliyatı). Poliplerden kanser gelişim riski düşük orandadır. Özellikle kanamaya sebep olan poliplerin alınması gereklidir.