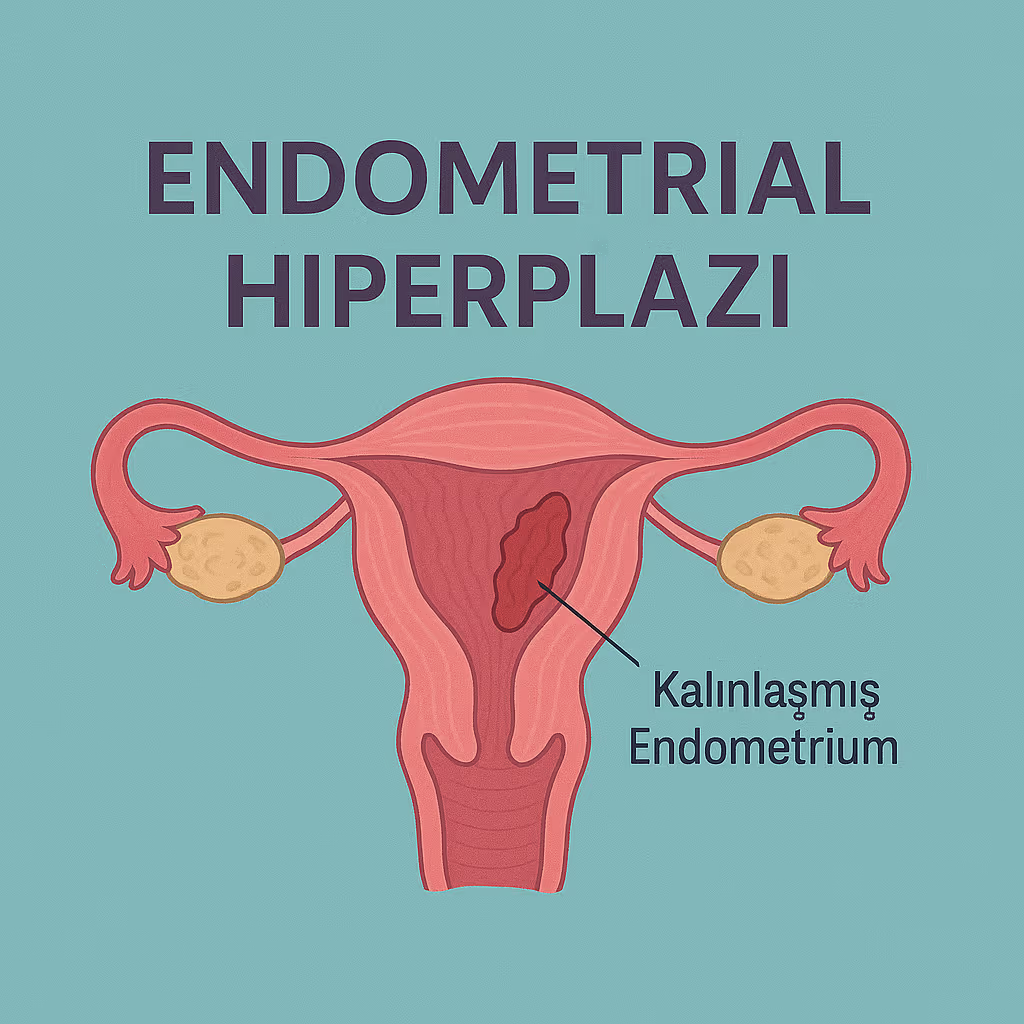
Endometrial Hiperplazi: Rahim İç Zarı Kalınlaşması Nedir?
Endometrial hiperplazi, halk arasında daha çok rahim iç zarı kalınlaşması olarak bilinen bir durumdur. Rahmin iç yüzeyini döşeyen dokuya endometrium denir. Bu doku, adet döngüsü boyunca hormonların etkisiyle kalınlaşır ve gebelik oluşmazsa adet kanamasıyla birlikte dökülür.
Ancak bazı durumlarda endometrium, normalden fazla ve düzensiz şekilde kalınlaşabilir. Bu duruma endometrial hiperplazi adı verilir. Endometrial hiperplazi çoğu zaman iyi huylu bir süreçtir; fakat bazı tipleri ilerleyen yıllarda rahim kanseri açısından risk oluşturabileceği için doğru tanı, uygun tedavi ve düzenli takip önemlidir.
Rahim iç zarı neden kalınlaşır?
Endometrium esas olarak iki önemli hormonun etkisi altındadır: östrojen ve progesteron.
Östrojen, rahim iç zarının kalınlaşmasını sağlar. Progesteron ise bu kalınlaşmayı dengeler ve dokunun düzenli biçimde olgunlaşmasına yardımcı olur. Eğer vücutta uzun süre östrojen etkisi baskın kalır, buna karşılık yeterli progesteron etkisi olmazsa endometrium kontrolsüz şekilde kalınlaşabilir.
Bu durum özellikle şu hallerde görülebilir:
Yumurtlamanın düzenli olmadığı adet döngüleri
Polikistik over sendromu
Obezite
Menopoza geçiş dönemi
Uzun süre adet görememe veya seyrek adet görme
Sadece östrojen içeren hormon tedavileri
Tamoksifen kullanımı
Diyabet, insülin direnci veya metabolik risk faktörleri
Ailede rahim, yumurtalık veya bağırsak kanseri öyküsü
Her rahim iç zarı kalınlaşması tehlikeli midir?
Hayır. Ultrasonografide rahim iç zarının kalın görünmesi tek başına kanser anlamına gelmez. Endometrium kalınlığı; yaşa, adet döngüsünün gününe, menopoz durumuna, kullanılan ilaçlara ve eşlik eden hastalıklara göre değişebilir.
Burada önemli olan şudur:
Kalınlaşmanın nedeni nedir ve hücrelerde atipi denilen anormal değişiklik var mıdır?
Endometrial hiperplazi genel olarak iki ana grupta değerlendirilir:
1. Atipisiz endometrial hiperplazi
Bu grupta rahim iç zarı hücreleri artmıştır, ancak hücrelerde belirgin kanser öncüsü yapısal bozulma yoktur. Atipisiz hiperplazi çoğu hastada tedaviyle veya bazı seçilmiş durumlarda yakın takip altında kendiliğinden gerileyebilir.
Kanserleşme riski düşüktür, ancak tamamen ihmal edilmemelidir. Çünkü devam eden anormal kanama, risk faktörlerinin sürmesi veya takipte gerileme olmaması durumunda tedavi planı yeniden değerlendirilmelidir.
2. Atipili endometrial hiperplazi / EIN
Atipili endometrial hiperplazi, güncel sınıflamalarda çoğu zaman EIN, yani endometrial intraepitelyal neoplazi kavramıyla birlikte ele alınır. Bu durumda hücrelerde daha belirgin anormallikler vardır ve rahim kanseri gelişme riski daha yüksektir.
Bu nedenle atipili hiperplazi, atipisiz hiperplaziye göre daha ciddi değerlendirilir. Tedavi planı yapılırken hastanın yaşı, çocuk isteği, ameliyat için uygunluğu ve eşlik eden risk faktörleri birlikte ele alınır.
Hangi belirtiler rahim iç zarı kalınlaşmasını düşündürür?
Endometrial hiperplazinin en sık belirtisi anormal rahim kanamasıdır.
Aşağıdaki durumlarda kadın hastalıkları ve doğum uzmanına başvurmak gerekir:
Adetlerin normalden çok daha yoğun olması
Adetlerin uzun sürmesi
İki adet arasında kanama olması
Düzensiz, sık veya beklenmedik kanamalar
Uzun süre adet görmedikten sonra kanama başlaması
Menopoz sonrası herhangi bir vajinal kanama olması
Lekelenme tarzında da olsa menopoz sonrası kanama görülmesi
Özellikle şu soru önemlidir:
Menopoz sonrası kanama normal midir?
Hayır. Menopoz sonrası kanama, miktarı az bile olsa normal kabul edilmez. Her menopoz sonrası kanama kanser anlamına gelmez; polip, atrofi, ilaç kullanımı veya iyi huylu nedenler de kanama yapabilir. Ancak rahim iç zarı hastalıklarının dışlanması için mutlaka değerlendirme gerekir.
Tanı nasıl konur?
Endometrial hiperplazi tanısı yalnızca ultrasonla kesinleştirilemez. Ultrason, rahim iç zarının kalınlığı ve rahim içi yapılar hakkında bilgi verir; ancak hücrelerin yapısını göstermez.
Kesin tanı için genellikle endometrial biyopsi, yani rahim iç zarından doku örneği alınması gerekir.
Tanıda kullanılan başlıca yöntemler şunlardır:
Transvajinal ultrasonografi
Vajinal ultrason ile rahim, yumurtalıklar ve rahim iç zarı değerlendirilir. Endometrium kalınlığı ölçülür. Ayrıca polip, miyom, sıvı birikimi veya rahim içi düzensizlik gibi durumlar araştırılır.
Üreme çağındaki kadınlarda endometrium kalınlığı adet döngüsüne göre değişebilir. Bu nedenle tek bir ölçüm her zaman hastalık anlamına gelmez. Menopoz sonrası dönemde ise rahim iç zarının kalınlığı daha dikkatli yorumlanır.
Endometrial biyopsi
Endometrial biyopsi, rahim iç zarından küçük bir doku örneği alınması işlemidir. Çoğu zaman muayenehane veya poliklinik şartlarında yapılabilir. Alınan örnek patoloji laboratuvarında incelenir.
Patoloji sonucu bize şu soruların yanıtını verir:
Hiperplazi var mı?
Varsa atipili mi, atipisiz mi?
Eşlik eden kanser bulgusu var mı?
Polip veya başka bir endometrial patoloji var mı?
Histeroskopi
Histeroskopi, rahim içine ince bir kamera sistemiyle bakılmasıdır. Özellikle rahim içinde polip, odak şeklinde kalınlaşma, düzensiz alan veya biyopsinin yetersiz olduğu durumlarda değerlidir.
Histeroskopi sırasında şüpheli alanlardan hedeflenmiş biyopsi alınabilir. Eğer polip saptanırsa aynı seansta çıkarılması da mümkün olabilir.
Her hastaya aynı tedavi mi uygulanır?
Hayır. Endometrial hiperplazide tedavi; hiperplazinin tipine, hastanın yaşına, menopoz durumuna, çocuk isteğine, kanama şikâyetine, risk faktörlerine ve patoloji sonucuna göre kişiselleştirilir.
Tedavide ana amaçlar şunlardır:
Anormal kanamayı kontrol altına almak
Rahim iç zarındaki kalınlaşmayı geriletmek
Kanser gelişme riskini azaltmak
Hastanın doğurganlık beklentisini dikkate almak
Tekrarlama riskini azaltmak
Atipisiz endometrial hiperplazide tedavi
Atipisiz hiperplazide bazı hastalar yakın takip ve risk faktörlerinin düzeltilmesiyle izlenebilir. Ancak kanaması olan, risk faktörleri devam eden veya takipte gerileme göstermeyen hastalarda progesteron tedavileri tercih edilir.
Progesteron tedavisi iki ana şekilde uygulanabilir:
Rahim içi progesteron sistemi
Levonorgestrel içeren rahim içi sistem, yani hormonlu spiral, birçok kılavuzda atipisiz endometrial hiperplazide ilk seçeneklerden biri olarak kabul edilir. Rahim içine doğrudan progesteron etkisi sağlar. Kanama miktarını azaltabilir, rahim iç zarının incelmesine yardımcı olabilir ve uzun süreli koruyucu etki sağlayabilir.
Ağızdan progesteron tedavisi
Bazı hastalarda ağızdan progesteron içeren ilaçlar kullanılabilir. Bu tedavilerin düzenli ve yeterli süre kullanılması önemlidir. Tedavinin tipi, dozu ve süresi hekim tarafından hastanın durumuna göre belirlenmelidir.
Atipisiz hiperplazide tedavi genellikle en az birkaç ay sürer ve yanıt, tekrar biyopsi ile değerlendirilir.
Kilo kontrolü neden önemlidir?
Yağ dokusu, vücutta östrojen etkisini artırabilen hormonal süreçlere katkıda bulunabilir. Bu nedenle fazla kilo veya obezite, endometrial hiperplazi riskini artırabilir ve tedavi sonrası tekrarlama ihtimalini yükseltebilir.
Kilo kontrolü, düzenli fiziksel aktivite, insülin direncinin yönetimi ve metabolik hastalıkların tedavisi yalnızca genel sağlık için değil, rahim iç zarı sağlığı için de önemlidir.
Atipili endometrial hiperplazide tedavi
Atipili hiperplazi veya EIN saptandığında yaklaşım daha dikkatli olmalıdır. Çünkü bu durumda rahim kanseri gelişme riski daha yüksektir ve bazı hastalarda tanı anında rahim içinde odak halinde kanser bulunma ihtimali de vardır.
Çocuk isteği tamamlanmış ve ameliyata uygun hastalarda çoğu zaman rahmin alınması, yani histerektomi, kesin tedavi olarak önerilir.
Ancak genç yaşta olan, çocuk sahibi olmak isteyen veya ameliyat için uygun olmayan hastalarda doğurganlığı koruyucu tedavi seçenekleri değerlendirilebilir. Bu durumda progesteron tedavisi uygulanabilir; fakat yakın takip şarttır. Takipte düzenli biyopsilerle hastalığın gerileyip gerilemediği kontrol edilir.
Histerektomi ne zaman gündeme gelir?
Histerektomi, yani rahmin cerrahi olarak alınması, her endometrial hiperplazi hastası için ilk seçenek değildir. Özellikle atipisiz hiperplazide çoğu hasta ilaç tedavisi ve takip ile yönetilebilir.
Ancak şu durumlarda cerrahi tedavi gündeme gelebilir:
Atipili hiperplazi / EIN saptanması
Çocuk isteğinin tamamlanmış olması
İlaç tedavisine rağmen gerileme olmaması
Tedavi sonrası hastalığın tekrarlaması
Kanamanın devam etmesi
Hastanın düzenli biyopsi takibini sürdürememesi
Eşlik eden başka rahim hastalıklarının bulunması
Menopoz sonrası dönemde yapılacak cerrahinin kapsamı, yumurtalık ve tüplerin alınıp alınmayacağı gibi ayrıntılar hastaya göre planlanır.
Tedavi sonrası takip nasıl yapılır?
Endometrial hiperplazide tedavi kadar takip de önemlidir. Çünkü hiperplazi gerileyebilir, devam edebilir veya bazı hastalarda tekrarlayabilir.
Atipisiz hiperplazide genellikle belirli aralıklarla endometrial biyopsi yapılır. Amaç, rahim iç zarının normale döndüğünü patolojik olarak göstermektir. Çoğu yaklaşımda iki ardışık negatif biyopsi sonrası takip aralığı azaltılabilir veya hasta izlemden çıkarılabilir.
Tekrarlama riski yüksek olan hastalarda daha uzun süreli takip gerekebilir. Özellikle vücut kitle indeksi yüksek olan, ağızdan progesteron tedavisi alan veya risk faktörleri devam eden hastalarda yıllık kontroller önerilebilir.
Atipili hiperplazi veya EIN nedeniyle rahim koruyucu tedavi alan hastalarda takip çok daha yakın yapılır. Bu hastalarda birkaç ay aralıklarla biyopsi tekrarlanması gerekebilir.
Tedavi bittikten sonra tekrar kanama olursa ne yapılmalı?
Tedavi tamamlandıktan ve kontroller normal çıktıktan sonra yeniden anormal kanama başlarsa bu durum ihmal edilmemelidir. Özellikle menopoz sonrası dönemde tekrar eden kanama, yeniden değerlendirme gerektirir.
Hastanın daha önce hiperplazi tanısı almış olması, yeni kanamanın mutlaka ciddiye alınmasını gerektirir.
Sık sorulan sorular
Rahim iç zarı kalınlaşması kanser midir?
Hayır. Endometrial hiperplazi kanser değildir. Ancak bazı tipleri, özellikle atipili hiperplazi veya EIN, rahim kanseri açısından daha yüksek risk taşır. Bu nedenle patoloji sonucu çok önemlidir.
Ultrason sonucunda endometrium kalın çıktı, hemen biyopsi gerekir mi?
Her zaman değil. Karar; yaşa, adet düzenine, menopoz durumuna, kanama şikâyetine, endometrium kalınlığına ve risk faktörlerine göre verilir. Menopoz sonrası kanama varsa değerlendirme daha acil ve dikkatli yapılır.
Hormonlu spiral herkese uygun mudur?
Hayır. Hormonlu rahim içi sistem birçok hastada etkili bir seçenektir; ancak rahim yapısı, enfeksiyon durumu, kanama nedeni, hastanın tercihi ve eşlik eden hastalıklar dikkate alınmalıdır.
Biyopsi ağrılı mıdır?
Bazı hastalar biyopsiyi hafif kramp şeklinde hissederken, bazı hastalarda daha belirgin ağrı olabilir. İşlem öncesi ağrı kesici, lokal yöntemler, sedasyon veya anestezi seçenekleri hastaya göre değerlendirilebilir.
Endometrial hiperplazi tekrarlar mı?
Evet, bazı hastalarda tekrarlayabilir. Risk faktörlerinin devam etmesi, obezite, düzensiz yumurtlama, tedaviye uyumsuzluk veya yetersiz takip tekrarlama riskini artırabilir.
Ne zaman doktora başvurmalıyım?
Aşağıdaki durumlarda kadın hastalıkları ve doğum uzmanına başvurmanız önerilir:
Menopoz sonrası kanama
Düzensiz ve sık kanama
İki adet arası kanama
Uzun süren veya aşırı adet kanaması
Uzun süre adet görmeme sonrası kanama
Daha önce endometrial hiperplazi tanısı alıp tekrar kanama yaşama
Polikistik over sendromu, obezite veya tamoksifen kullanımı gibi risk faktörleriyle birlikte kanama düzensizliği
Sonuç
Endometrial hiperplazi, yani rahim iç zarı kalınlaşması, doğru değerlendirildiğinde çoğu zaman yönetilebilir bir durumdur. Ancak tanının netleştirilmesi, atipi varlığının belirlenmesi ve uygun takip planının yapılması çok önemlidir.
Her hastanın tedavi planı aynı değildir. Bazı hastalarda takip yeterli olabilirken, bazılarında progesteron tedavisi, hormonlu rahim içi sistem veya cerrahi tedavi gerekebilir.
Özellikle menopoz sonrası kanama, tekrarlayan düzensiz kanama veya risk faktörleri bulunan hastalarda gecikmeden uzman değerlendirmesi yapılmalıdır. Erken tanı ve düzenli takip, hem gereksiz endişeyi azaltır hem de ciddi hastalıkların erken dönemde yakalanmasını sağlar