Endometrial Biyopsi (Probe / Pipelle Biyopsi) Nedir?
Endometrial biyopsi, rahmin iç tabakası olan endometriumdan küçük bir doku örneği alınarak mikroskop altında incelenmesini sağlayan tanısal bir işlemdir. Halk arasında bazen “rahimden parça alınması”, “probe biyopsi” veya “pipelle biyopsi” olarak da ifade edilir.
Bu işlem genellikle poliklinik şartlarında, kısa sürede yapılabilir. Amaç; anormal kanamanın nedenini araştırmak, endometriumda kalınlaşma, polip, hiperplazi, enfeksiyon veya kanser öncüsü/kanser hücreleri olup olmadığını değerlendirmektir.
“Her kanama biyopsi gerektirir mi?”
Hayır. Her adet düzensizliği veya kanama endometrial biyopsi gerektirmez. Ancak bazı kanama tipleri daha dikkatli değerlendirilmelidir:
Menopoz sonrası kanama
Adetler arasında kanama
Cinsel ilişki sonrası kanama
Uzun süren veya aşırı miktarda adet kanaması
Düzensiz, sık veya beklenmedik kanamalar
Tedaviye rağmen devam eden kanama
Rahim iç tabakasında ultrasonla kalınlaşma saptanması
Endometrial hiperplazi veya kanser açısından risk faktörlerinin bulunması
Özellikle menopoz sonrası kanama, miktarı az bile olsa mutlaka jinekolojik değerlendirme gerektirir.
Endometrial Biyopsi Neden Yapılır?
Endometrial biyopsi en sık şu durumlarda istenir:
1. Anormal Uterin Kanama
Adet düzeninden farklı, beklenmedik veya aşırı kanamalar “anormal uterin kanama” olarak değerlendirilir. Bu durum hormonal düzensizliklerden poliplere, miyomlardan endometrial hiperplaziye kadar birçok nedenle ortaya çıkabilir.
2. Menopoz Sonrası Kanama
Menopozdan sonra görülen vajinal kanama normal kabul edilmez. Sebep çoğu zaman iyi huylu olabilir; ancak endometrial kanser veya kanser öncüsü değişiklikleri dışlamak için değerlendirme gerekir.
3. Endometrial Kalınlaşma
Ultrasonografide rahim iç tabakasının beklenenden kalın görülmesi durumunda biyopsi gerekebilir. Ancak karar yalnızca kalınlık ölçümüne göre değil; hastanın yaşı, menopoz durumu, kanama öyküsü, ilaç kullanımı ve risk faktörleri birlikte değerlendirilerek verilir.
4. Endometrial Hiperplazi Şüphesi
Endometrial hiperplazi, rahim iç tabakasının normalden fazla kalınlaşmasıdır. Bazı tipleri kanser öncüsü kabul edilebilir. Biyopsi, hiperplazinin tipini ve atipi olup olmadığını ayırt etmede önemlidir.
5. Tedaviye Yanıtın Takibi
Daha önce endometrial hiperplazi tanısı almış hastalarda, hormon tedavisi veya diğer tedaviler sonrası rahim iç tabakasının tedaviye yanıtını değerlendirmek için tekrar biyopsi yapılabilir.
“Biyopsi kanser olduğum anlamına mı gelir?”
Hayır. Biyopsi yapılması, hastada kesin olarak kanser olduğu anlamına gelmez. Endometrial biyopsi bir tanı koyma veya ciddi hastalıkları dışlama yöntemidir. Çoğu hastada sonuç iyi huylu değişiklikler, hormonal etkiler, polip, atrofi veya enfeksiyon gibi nedenleri gösterebilir.
Ancak biyopsinin önemli avantajı, endometrial hiperplazi ve endometrial kanser gibi erken tanı gerektiren durumların saptanmasına yardımcı olmasıdır.
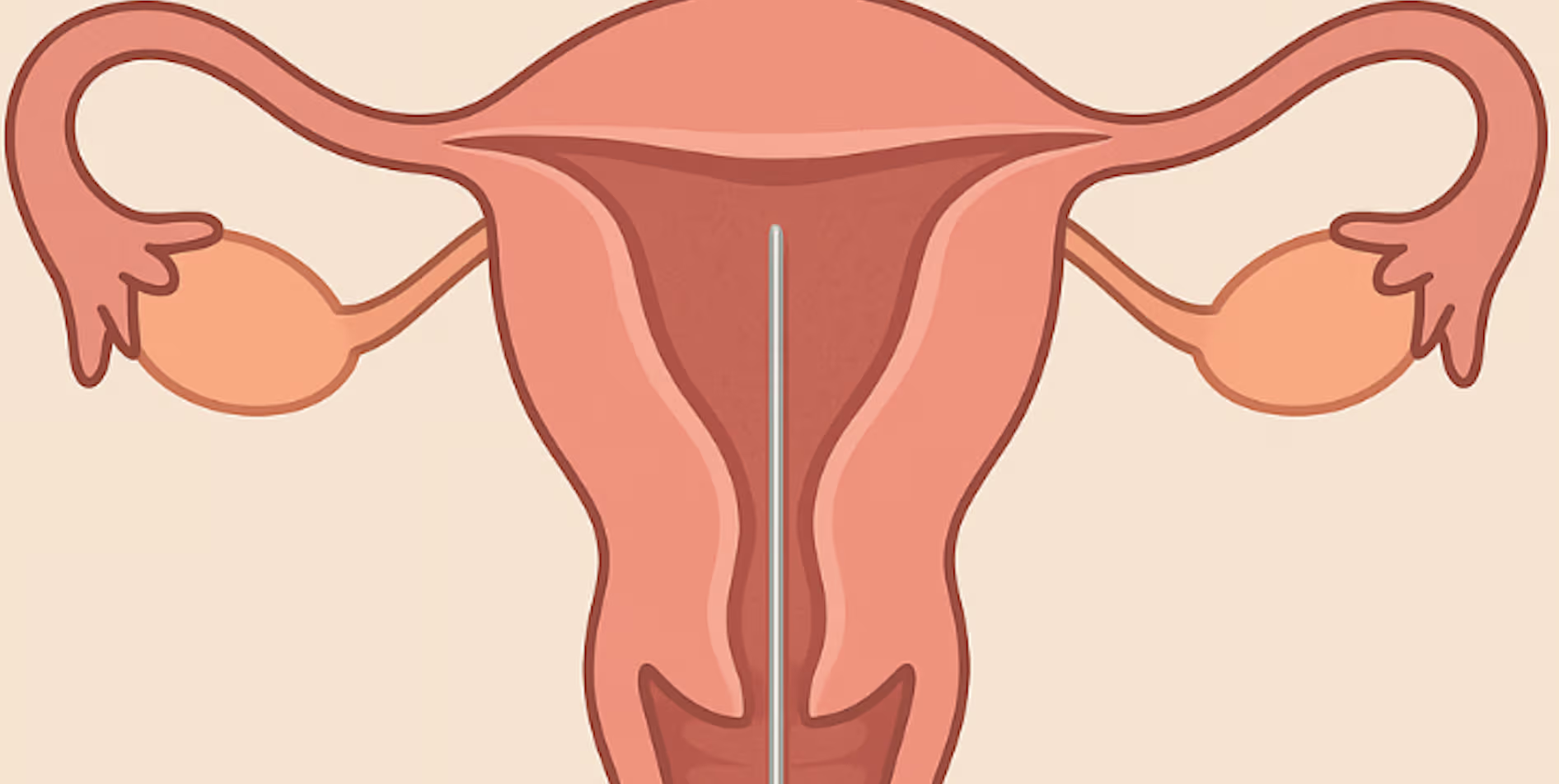
İşlem Nasıl Yapılır?
Endometrial biyopsi genellikle jinekolojik muayene pozisyonunda yapılır.
Vajinaya spekulum yerleştirilir.
Rahim ağzı görünür hale getirilir.
İnce, esnek bir biyopsi kanülü rahim ağzından geçirilerek rahim içine ulaştırılır.
Rahim iç tabakasından küçük doku örnekleri alınır.
Alınan örnek patoloji laboratuvarına gönderilir.
İşlem çoğu zaman birkaç dakika sürer. Bazı hastalar işlem sırasında adet sancısına benzer kramp hissedebilir. Bu his genellikle kısa sürelidir.
“Endometrial biyopsi ağrılı mıdır?”
Ağrı kişiden kişiye değişir. Bazı hastalar hafif bir rahatsızlık hissederken, bazı hastalarda kısa süreli ancak daha belirgin kramp olabilir. İşlem öncesinde doktorunuz uygun görürse ağrı kesici kullanımı, lokal uygulamalar veya farklı ağrı kontrol yöntemleri değerlendirilebilir.
Daha önce zor jinekolojik muayene geçirmiş, rahim ağzı darlığı olan, doğum yapmamış veya ağrı eşiği düşük olan hastalarda işlem planlaması kişiye özel yapılmalıdır.
İşlem Öncesi Nelere Dikkat Edilmelidir?
İşlem öncesinde doktorunuza şu bilgileri mutlaka vermelisiniz:
Gebelik ihtimali
Kan sulandırıcı ilaç kullanımı
Kanama bozukluğu öyküsü
İlaç, lateks veya antiseptik alerjisi
Aktif vajinal enfeksiyon belirtileri
Daha önce geçirilmiş rahim, rahim ağzı veya pelvik cerrahiler
Spiral veya rahim içi araç kullanımı
Gebelik varsa veya gebelik ihtimali dışlanmamışsa endometrial biyopsi genellikle yapılmaz.
Biyopsi Sonrası Neler Normaldir?
İşlem sonrası kısa süreli hafif kramp, lekelenme tarzı kanama veya kahverengi akıntı görülebilir. Bu belirtiler genellikle birkaç gün içinde azalır.
Doktorunuz farklı bir öneride bulunmadıysa çoğu hasta günlük hayatına kısa sürede dönebilir. Ancak işlemden sonra ağır egzersiz, cinsel ilişki, tampon kullanımı veya vajinal duş konusunda doktorunuzun önerilerine uymanız önemlidir.
Ne Zaman Doktora Başvurulmalıdır?
Biyopsi sonrası aşağıdaki durumlarda gecikmeden doktorunuza başvurmalısınız:
Yoğun veya durmayan kanama
Kötü kokulu vajinal akıntı
Ateş veya titreme
Şiddetli kasık/karın ağrısı
Bayılma hissi, baş dönmesi
Ağrı kesiciye rağmen geçmeyen ağrı
Bu bulgular enfeksiyon, yoğun kanama veya nadir komplikasyonlar açısından değerlendirme gerektirebilir.
Endometrial Biyopsi Sonucu Nasıl Yorumlanır?
Patoloji sonucu genellikle birkaç başlık altında değerlendirilir:
Normal veya Benign Bulgular
Rahim iç tabakasında kanser veya kanser öncüsü değişiklik saptanmayabilir. Kanama şikâyeti devam ediyorsa altta yatan hormonal nedenler, polip, miyom veya başka jinekolojik durumlar ayrıca araştırılabilir.
Endometrial Polip
Polipler rahim iç tabakasından gelişen çoğu zaman iyi huylu oluşumlardır. Kanama, lekelenme veya infertiliteyle ilişkili olabilir. Tedavide histeroskopik çıkarma düşünülebilir.
Endometrit
Rahim iç tabakasında iltihabi değişiklik saptanabilir. Bu durumda antibiyotik tedavisi veya ek değerlendirme gerekebilir.
Endometrial Hiperplazi
Hiperplazinin atipili veya atipisiz olması tedavi planını değiştirir. Atipisiz hiperplazide progesteron tedavileri ve düzenli takip tercih edilebilir. Atipili hiperplazi daha yakın takip ve bazı hastalarda cerrahi değerlendirme gerektirebilir.
Endometrial Kanser
Kanser saptanması durumunda hasta jinekolojik onkoloji açısından değerlendirilir. Tedavi; hastalığın tipine, evresine, hastanın yaşı ve genel sağlık durumuna göre planlanır.
Yetersiz Materyal
Bazen alınan doku tanı için yeterli olmayabilir. Bu durumda biyopsinin tekrarı, ultrasonografi, histeroskopi veya küretaj gibi ek yöntemler gerekebilir.
“Biyopsi normal çıkarsa her şey kesin olarak bitti mi?”
Normal biyopsi sonucu rahatlatıcıdır; ancak şikâyetlerin devam etmesi halinde değerlendirme sürmelidir. Çünkü bazı odak lezyonlar, örneğin polipler veya sınırlı alanlardaki değişiklikler, kör biyopsi ile her zaman yakalanamayabilir. Devam eden kanama, tekrarlayan lekelenme veya ultrasonografide şüpheli bulgu varsa histeroskopi gibi rahim içini doğrudan görmeye olanak sağlayan yöntemler gerekebilir.
Tanıda Hangi Yöntemler Birlikte Kullanılır?
Endometrial biyopsi çoğu zaman tek başına değil, diğer değerlendirme yöntemleriyle birlikte ele alınır:
Jinekolojik muayene
Transvajinal ultrasonografi
Gebelik testi
Kan sayımı
Hormon testleri
Pap smear veya HPV testi, gerektiğinde
Histeroskopi
Salin infüzyon sonografi
Gerektiğinde MR veya ileri görüntüleme
Hangi testlerin gerekli olduğu hastanın yaşı, şikâyeti, menopoz durumu ve muayene bulgularına göre belirlenir.
Tedavi Yöntemleri Nelerdir?
Endometrial biyopsi bir tedavi değil, tanı yöntemidir. Tedavi, biyopsi sonucuna ve altta yatan nedene göre planlanır.
Hormonal Düzensizliklerde
Progesteron içeren ilaçlar, kombine hormonal tedaviler veya hormonlu spiral gibi seçenekler değerlendirilebilir.
Polip veya Submuköz Miyom Varsa
Histeroskopi ile rahim içi lezyonun çıkarılması gerekebilir.
Endometrial Hiperplazide
Atipisiz hiperplazide progesteron tedavisi ve düzenli biyopsi/ultrason takibi uygulanabilir. Atipili hiperplazide hastanın çocuk isteği, yaşı ve risk durumu dikkate alınarak daha ileri tedavi seçenekleri gündeme gelebilir.
Enfeksiyon Varsa
Uygun antibiyotik tedavisi planlanır.
Kanser Saptanırsa
Jinekolojik onkoloji değerlendirmesi yapılır. Tedavi genellikle cerrahi temellidir; ancak hastalığın evresine ve tipine göre radyoterapi, kemoterapi veya hormon tedavileri de gündeme gelebilir.
Takip Nasıl Yapılır?
Takip planı biyopsi sonucuna göre değişir.
Sonuç normal ve şikâyetler geçmişse rutin takip yeterli olabilir.
Kanama devam ediyorsa ileri değerlendirme gerekebilir.
Hiperplazi saptandıysa belirli aralıklarla kontrol biyopsisi veya görüntüleme yapılabilir.
Polip veya miyom tedavisi sonrası semptomların tekrarlayıp tekrarlamadığı izlenir.
Kanser tanısında takip, jinekolojik onkoloji protokollerine göre planlanır.
Sık Sorulan Sorular
İşlemden sonra çalışabilir miyim?
Çoğu hasta aynı gün günlük yaşamına dönebilir. Ancak ağrı, kramp veya kanama varsa dinlenmek daha uygun olabilir.
Biyopsi doğurganlığı etkiler mi?
Standart endometrial biyopsinin doğurganlığı kalıcı olarak bozması beklenmez. Ancak biyopsi sonucunda saptanan hastalıklar veya yapılacak tedaviler doğurganlık açısından ayrıca değerlendirilmelidir.
Biyopsi yerine ultrason yeterli midir?
Ultrason rahim iç tabakası hakkında önemli bilgi verir; ancak hücresel tanı koyamaz. Kanser öncüsü değişiklikler veya kanser şüphesinde doku tanısı gerekir.
Probe biyopsi ile kürtaj aynı şey midir?
Hayır. Probe/pipelle biyopsi genellikle ince bir kanülle sınırlı doku örneği alınmasıdır. Küretaj ise rahim içinden daha geniş örnekleme yapılmasını içeren farklı bir işlemdir ve çoğu zaman anestezi altında uygulanabilir.
Sonuç
Endometrial biyopsi, anormal rahim kanamalarının ve rahim iç tabakasına ait hastalıkların değerlendirilmesinde önemli, kısa süreli ve çoğu zaman poliklinik şartlarında yapılabilen bir tanı yöntemidir. Amaç yalnızca kanser araştırmak değil; kanamanın nedenini anlamak, doğru tedaviyi planlamak ve gerektiğinde hastayı güvenli şekilde takip etmektir.
Her hastanın durumu farklıdır. Bu nedenle biyopsi gerekliliği, işlem şekli, sonuçların yorumu ve takip planı mutlaka kişiye özel olarak kadın hastalıkları ve doğum uzmanı tarafından değerlendirilmelidir.